Medical Support
(Non-Invasive Cardiovascular Care)
We provide non-invasive ECP Therapy and advanced diagnostics to support circulation and cardiovascular function. Our approach is structured and assessment-led, with a focus on clear education, careful screening, and personalised planning.
ECP Therapy is clinically studied and is used internationally in cardiovascular and cardiac rehabilitation settings. It may help reduce symptoms associated with heart disease and chronic stable angina for suitable clients, and may support improved exercise tolerance, functional capacity, and day-to-day capacity. For more on the research, see our Clinical Studies page.

Conditions we commonly support
(where clinically appropriate)
Heart disease and chronic stable angina
Cardiovascular conditions affecting circulation and exercise tolerance
Fatigue associated with reduced cardiovascular function
Rehabilitation following cardiac events, where appropriate
How ECP Therapy works (plain language)
ECP Therapy uses timed inflation and deflation of cuffs on the legs to support blood flow back toward the heart at specific points in the heartbeat cycle. This can support circulation efficiency and vascular function.
Cardiac Rehabilitation and Function (where appropriate)
For suitable clients, ECP Therapy may also be used as a supportive tool within cardiac rehabilitation and broader rehabilitation plans. By supporting circulation and recovery capacity, it may help some people tolerate rehabilitation better and progress more consistently toward a graded return to activity or work.
Diagnostics and Assessment
Where appropriate, we use non-invasive testing to establish a baseline and guide planning. Diagnostic ultrasound is available on the premises to support assessment and rehabilitation planning.
Evidence and Research
ECP Therapy has been studied internationally. During your consultation, we can explain the evidence in plain language, discuss suitability and contraindications, and outline what outcomes are realistic for your situation.
BOOK NOW FOR AN ECP THERAPY CONSULTATION
Hemodynamic Impact of ECP Therapy
Due to the hemodynamic effects of ECP, the benefits apply not only to the heart, but to the entire cardiovascular system. Enhanced blood circulation during the inflation and deflation of cuffs during the therapy, greatly increases shear stress (the frictional force on blood vessels), thereby stimulating production of Nitric Oxide.
Simultaneous deflation
- Decreased systemic vascular resistance (2)
- Decreased cardiac workload (3)
- Decreased myocardial oxygen consumption (2)
- Decreased after load (2)
Sequential inflation
- Retrograde aortic pressure wave (2)
- Increased diastolic pressure (2)
- Increased intracoronary perfusion pressure (2)
- Increased myocardial perfusion (2)
- Increased venous return (2)
- Increased preload (2)
- Increased cardiac output (2)
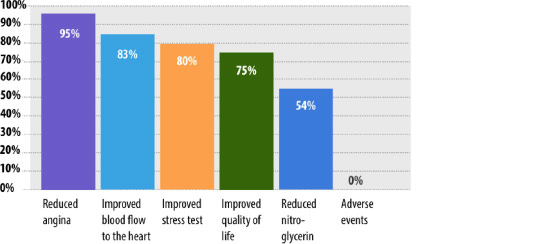
Effective and Proven
Here are some key findings from extensive research into how the integration of ECP therapy can improve the patient quality of life, reduce long term treatment costs and re-hospitalisation.
Clinical Effects of ECP
Nitrate use (4)

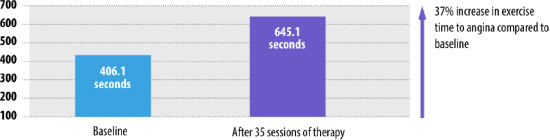
Improvement in time to angina during exercise (4)
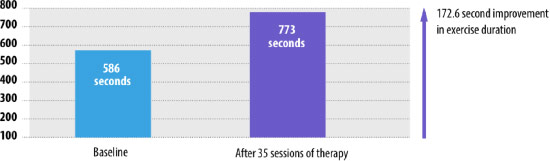
Improved exercise duration (4)
The benefits of therapy that last three or more years (1)
Additional benefits of ECP therapy
- Sustained improvements at three years in quality of life scores
- The frequency of angina reduced by four episodes per week immediately post-therapy and this was sustained at the three year follow-up.
Long-term follow-up from the IEPR CCS classification (1)
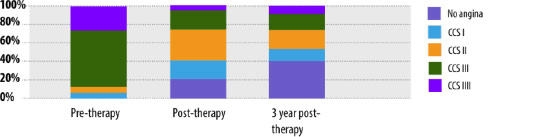
- 1,061 patients from 36 centres completed a three year follow-up.
- 9% of patients improved by at least on CCS classification.
Impact on hospitalisation
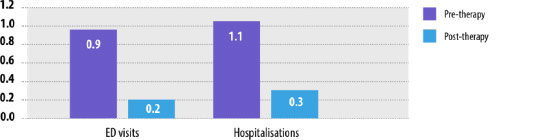
- ED visits and hospitalisations six-month follow-up (5) Significant reduction in rates of ED visits and hospitalisation compared to six month pre-treatment.
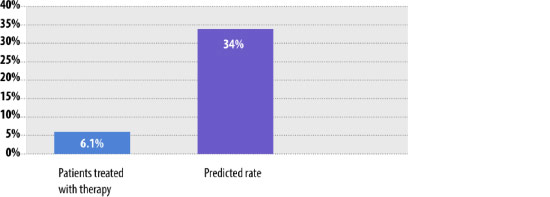
Impact of therapy on HF re-hospitalisations (6)
- Observed and predicted re-admissions rates for 90 days after discharge.
- Loh, et al. Enhanced External Counterpulsation in the Treatment of Chronic Refractory Angina: A Long-term Follow-up Outcome from the International Enhanced External Counterpulsation Patient Registry. Clin Cardiol. 2008;31:159-164. 2.Shea M, et al. An Update on Enhanced External Counterpulsation. Clin Cardiol. 2005;28,115–118. 3. Lloyd-Jones D, et al. Heart disease and stroke statistics—2010 update: a report from the American Heart Association. Circulation. 2010;121:e46–215. 4. Braith RW, et al. Enhanced external counterpulsation improves peripheral artery flow-mediated dilation in patients with chronic angina: a randomized sham-controlled study. Circulation. 2010;122:1612-20. 5. Soran O, et al. Impact of external counterpulsation treatment on emergency department visits and hospitalizations in refractory angina patients with left ventricular dysfunction. Congest Heart Fail. 2007;13:36-40. 6. Tecson K, et al. Impact of Enhanced External Counterpulsation on Heart Failure Rehospitalization in Patients with Ischemic Cardiomyopathy. Am J Cardiol. 2016;117:901-905.